OUR CASE
Matt was in ICU for a total of 10 days after his injury.
He then went to the spinal rehab ward with a C5 ASIA B SCI, so had good elbow flexion strength bilaterally.
While he was there, he had important logistics organised such as a customised motorised wheelchair he could control with a joystick allowing some independence of mobility.
He still needed assistance for all transfers and with all ADLs but could feed himself with a special splint.
Physio focused on his chest, needing cough assists and occasional more intensive physio when he had respiratory infections, as well as range of motion and stretching exercises to prevent elbow flexion and supination contractures.
Occupational therapy became involved and were integral to long term planning.
After a month he started to get problems with spasticity, which improved with increased oral baclofen.
He had orthostatic hypotension initially, so needed gradually increasing periods on a tilt table until this was no longer a problem.
He had urodynamic testing and an SPC was inserted at 7 weeks.
After 8 weeks he moved from acute to chronic spinal rehab; the aim was then to prepare him for discharge to the community.
He was in rehab for 7 months while a care package was organised and the necessary house modifications could be made.
During this time he became low in mood; this was greatly helped by the spinal psychologist and the occupational therapy team, and by the time he was discharged his mood was thought to be back to his baseline.
Patient outcomes
Hospital survival after SCI is now > 90%
Long-term survival is considerably better than 40 years ago
> NLOI
> Complete SCI
> Older age
> Comorbidities
> Best predictor is an accurate ISNCSCI
> ISNCSCI even in first 24 hours highly predictive of outcome
> Complete (ASIA A) injuries have least potential for recovery (7% improve to ASIA B by 1 year, virtually none become motor incomplete)
> Half ASIA B improve to ASIA C or D by 1 year
> Most initial ASIA C < 50 years and all ASIA D are expected to walk by discharge from rehab

> Several predictive findings on MRI T2 sequences; more points, worse prognosis REF:
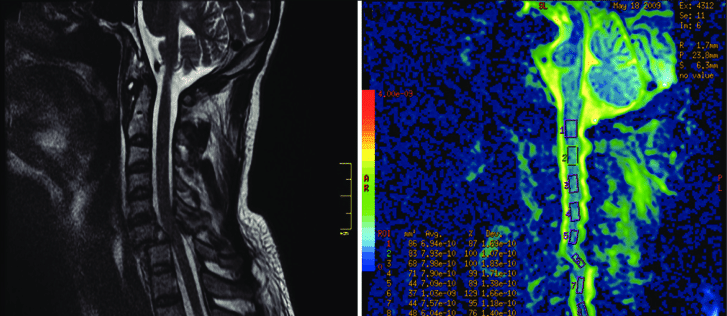
DT MRI
> Diffusion tensor Imaging sequences may be promising to predict outcome in both acute and chronic SCI patients
> For example fractional anisotropy in DTI may predict functional status of the cord.