
Cerebral blood volume increases with:
> Hypoxia (exponentially below PaO2 <50 mmHg)
> Hypercapnea (linearly between a range of PaCO2 20-80 mmHg)
> Increased cerebral metabolic rate
> Obstruction to venous drainage
CPP= MAP – ICP (or MAP – RAP)
Target CPP 60-70 mmHg in TBI
Target ICP <22 mmHg in TBI
Explore the relationship between pressure, volume and blood flow…
CEREBRAL BLOOD FLOW
The brain receives 15% of cardiac output under normal circumstances
This is 50 ml/100 g brain tissue/min
Cerebral oxygen consumption (CMRO2) comprises 20% of total body oxygen consumption.
Critical cerebral blood flow is around 20 ml/100 g/min, and below 15 ml/100 g/min the EEG becomes isoelectric.
The grey matter of the brain receives the majority of cerebral blood flow.
INTRACRANIAL PRESSURE
Under normal physiological conditions, the ICP ranges between 0-15 mmHg.
When straining this may increase to 50 mmHg without neurological injury.
CEREBRAL PERFUSION PRESSURE
The normal cerebral perfusion pressure (CPP) is 60 mmHg, maintained by autoregulation (see below)
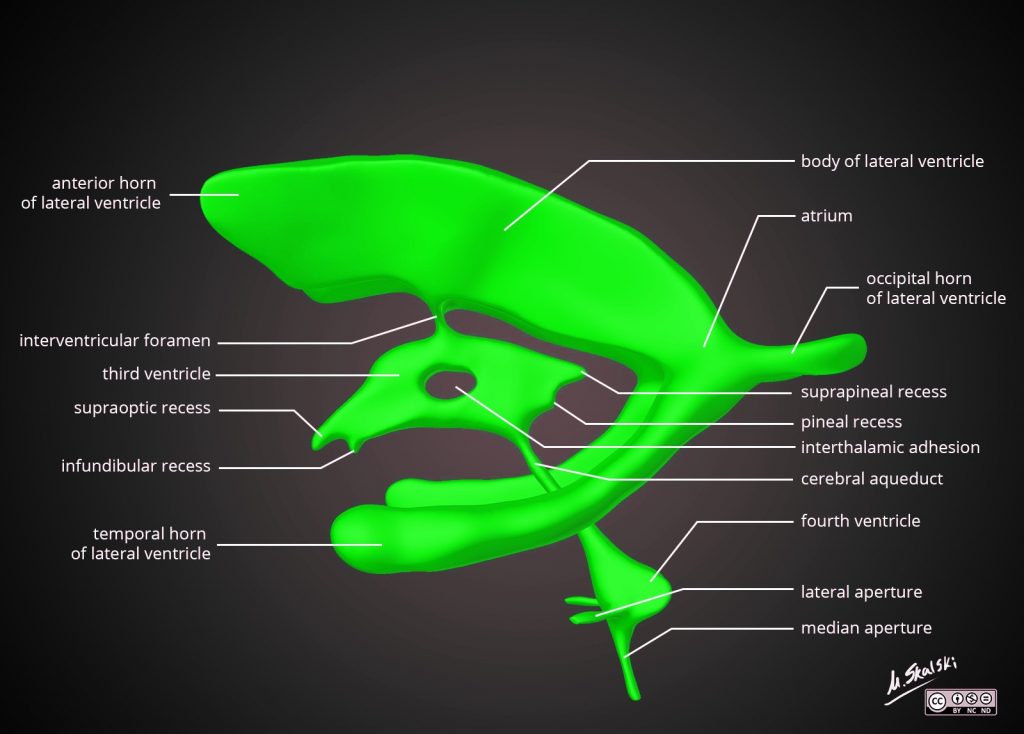
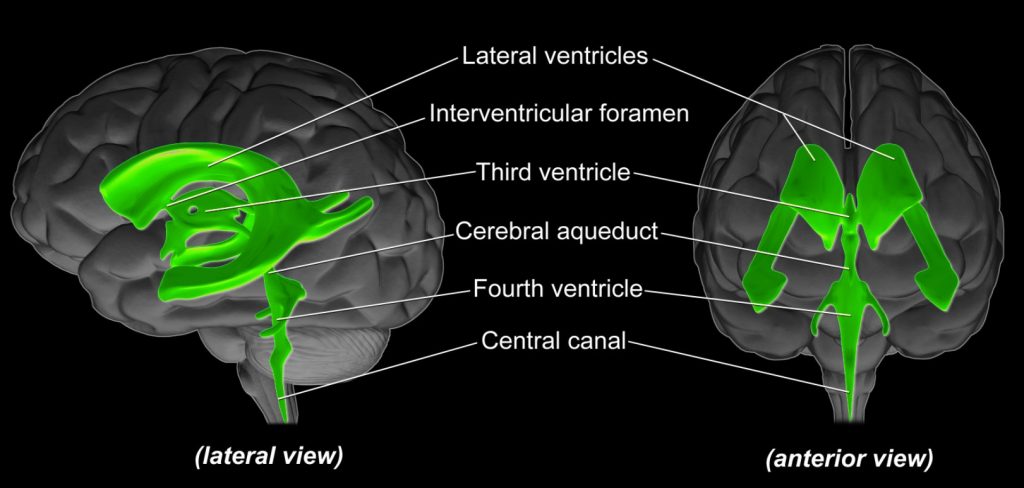
CEREBROSPINAL FLUID
The normal amount of cerebrospinal fluid in the body is approximately 150 ml, of which 75 ml exists intracranially, 75 ml in the spine.
CSF is formed at a rate of approximately 500-600 ml/day (turns over 3-4 times).
CSF is produced by active secretion and ultrafiltration.
70% of CSF is formed by the choroid plexus, a network of blood vessels covered by ependymal cells projecting into the ventricles.
30% is formed directly from the ependymal cells lining the capillaries of the ventricles.
CSF production is NOT regulated by intracranial pressure.
Ciliary action, arterial pulsation and normal respiration propels the CSF through the ventricles.
PRESSURE KILLS
We know, particularly from TBI experience:
High levels of ICP are associated with mortality REF
Even brief (>5 minutes) episodes of intracranial hypertension are associated with worse outcome REF
So avoiding intracranial hypertension is a key part of all TBI guidelines.
A threshold of 22 mmHg is used as a intervention trigger in the context of TBI
It should be noted that there’s lack of certainty about what thresholds of ICP justify therapies that have intrinsic toxicities (see later), and the definition of the critical “dose” of intracranial hypertension remains an important, but elusive, goal REF
NOT THE PRESSURE BUT THE FLOW
The most crucial factor for brain function and survival is adequate cerebral blood flow (CBF) to meet cerebral metabolic rate of oxygen consumption (CMRO2)
Cerebral blood flow can’t practically be measured at the bedside.
The surrogate we currently use is Cerebral Perfusion Pressure (CPP)
This is the difference between the blood pressure going into the head (mean arterial pressure, MAP, measured with transducer at the level of the Foramen of Monroe) and the pressure this encounters, i.e. the pressure in the head or the venous pressure on the other side.
In normal physiology, this is:
CPP = MAP – Right Atrial Pressure
In brain injury, intracranial pressure (ICP) often exceeds the venous pressure, so:
CPP = MAP – ICP
So you’ll see why we focus on either reducing the ICP or increasing the MAP
We also try to avoid factors that impede venous outflow such as:
- Bad head positioning
- Lying supine
- Tight ETT ties
- Cervical collars
- High PEEP
- Abdominal compartment syndrome
- Right heart failure
In TBI, we target a CPP of 60-70 mmHg
When measuring CPP, the MAP is read at the level of the brain, with the arterial line transducer at the level of the external auditory meatus (roughly the position of the Foramen of Monro).
IF CBF IS SO IMPORTANT, WHY DON’T WE WORRY ABOUT IT NORMALLY?
In health, CBF is auto-regulated to keep it normal over a blood pressure range of about MAP 60-160 mmHg
Auto regulation is local and systemic


{kind=link}
{kind=link}
{kind=link}
The Monroe-Kellie Hypothesis
Monro-Kellie Hypothesis
The cranial vault is a fixed volume space filled with three components:
- Brain parenchyma 85% / 1400 ml
- Cerebrospinal fluid 10% / 150 ml
- Intracranial blood 5% / 150 ml
As the cranial vault is a fixed volume space, an increase in volume of any of the three contents should cause a reciprocal decrease in one or both of the other two contents.
The only hole in an intact skull is at the bottom: the foramen magnum (FM)
If a haematoma, tumour or cerebral oedema represents a new volume and the pressure rises:
> First CSF can be displaced from the ventricles and subarachnoid spaces and exit the intracranial compartment via the FM
> Then intravenous blood can be displaced through the jugular foramina via the internal jugular veins
> Brain parenchyma can be pushed downward into the FM (cerebral herniation) although brain tissue cannot actually exit the skull
> As the pressure rises, arterial blood is displaced and CPP decreases, eventually producing diffuse cerebral ischemia.
> At pressures equal to mean arterial pressure, arterial blood is unable to enter the skull through the FM, producing complete cessation of blood flow to the brain, with resultant massive infarction and brain death
The context of EICP is important
For example, during CSF infusion studies in patients with hydrocephalus, saline is infused into cerebral ventricles of awake patients.
ICP is measured and often exceeds 40 mmHg(!) without causing symptoms or altered cerebral blood flow.
This is because there the buffering mechanisms are still intact so CSF can leave the skull, and cerebral pressure autoregulation maintains CBF over a wide range of CPP. REF
The extrapolation of this is that TBI patients with open basal cisterns and preserved pressure autoregulation are more likely to be able to tolerate transient elevations in ICP compared to those with more decompensated systems.
In these patients we reduce sedation to neurologically assess patients and expect / allow transient EICP with coughing and desynchrony with the ventilator.
Clearly patients with effaced basal cisterns (know your cisterns), compressed cortical sulci and midline shift are likely to have decompensated reserve and these are the patients where ICP must be aggressively controlled until this period has subsided, often days later.
Name as many causes of elevated intracranial pressure as you can